
RUSH Protocol
The Case
45 year old female presents to the ER with a chief complaint of light headedness. Ms. Lawson began experiencing these episodes yesterday morning. Episodes of pre-syncope (vision darkening, muscle weakness, and light headedness) are brought on by standing up and relieved by laying down. She denies palpitations, chest pain, dyspnea, fevers, recent illness, loss of consciousness, or confusion. She has never experienced anything like this before. She denies a history of cardiac disease or recent trauma. The patient has a past medical history of hypertension, hyperlipidemia, and obesity. Her current medications are lasix, metoprolol and atorvastatin. Her vitals are as follows: BP – 86/72, HR – 80, RR – 14, Temp – 37C, and O2 Sat – 95%. Her pupils are equal and reactive to light. CN II-XII are intact bilaterally. Her lung are clear to auscultation and her trachea is midline. There is no JVD, no tachycardia, no murmurs/rubs/gallops. Her ECG shows a regular sinus rhythm. Her abdomen is soft and non-tender with no palpable or pulsatile masses. Her peripheral pulses are present and equal. She has no pitting edema in her extremities.
You decide to perform a quick ultrasound examine to gather some more information. You complete the RUSH (rapid ultrasound for shock and hypotension) protocol to evaluate the patient’s undifferentiated hypotension. Below are your results.
Heart – Subcostal Cardiac

Heart – Parasternal Long Views

IVC – Saggital View
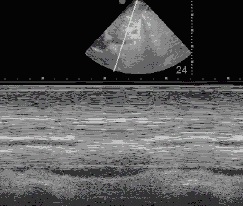
Morrison’s Pouch – RUQ View

Aorta – Tranverse View

Pulmonary (bilaterally) – Imaged Parasternally at 2nd Intercostal Space

Suggest Resources
Academic Life in EM: “RUSH protocol: Rapid Ultrasound for Shock and Hypotension”
Introduction to Bedside Ultrasound: Vol. 1, Ch. 5 “RUSH”
Mount Sinai Ultrasound: “RUSH“
The Quiz
CLICK HERE to take the quiz (and be entered to win some coffee!)

subaortic hypertrophic cardiomyopathy